
In this article, team members from BWBR and Dunham Associates explore performance design options for healthcare facilities operating during a pandemic. The team adapted concepts that were originally developed for Chasing 2030: Mechanical Strategies for Hospitals, a presentation developed for AIA Minnesota in 2015.
In August when nationally renowned University of Minnesota epidemiologist Michael Osterman, PhD, warned of a second wave of COVID-19 infections, his prediction landed as more than a call-to-action. It was also a reminder of the effects the pandemic had on hospitals and health systems, effects that exceeded an estimated $200 billion nationally in the first three months because of canceled non-emergent and postponed care. From supply chain disruptions to surge capacity and available local resources, Osterholm said there were key questions that administrators and managers needed to answer in preparing for the second wave.
The impact to finances for hospitals and health systems have been devastating for an industry whose median margins were 3.5% before the pandemic. See KaufmanHall’s The Effect of COVID-19 on Hospital Financial Health.
For rural and critical access hospitals, those margins were significantly smaller. Those tight margins always had teams looking for efficiencies, and with many efforts coming in the mechanical systems. As the pandemic put healthcare providers in crisis response mode to treat patients with COVID-19 and prevent the spread of the virus in their facilities, the focus shifted to the immediate conversion of spaces for safe treatment, with temporary ventilation strategies for negative air flow rooms and units, operational efficiencies aside.
Months into the pandemic, there is a shift in focus, from implementing CDC recommendations in preparation for a surge of patient cases to one that is more long-term, with an understanding that, in the new normal, “pandemic operations” will just be part of operations. As hospitals navigate past the immediate crisis, the new challenge is to find ways to create energy-efficient hospitals while planning for future pandemics.
Pushing the efficiency discussion pre-pandemic was not only cost reduction but also sustainability. The environmental impact of buildings and their operations is amplified by the spread of SARS-like viruses, with COVID-19 being the third to spread in the past 15 years. As researchers study such spread correlated to climate change and warming temperatures, there is no denying the impact a changing climate has on the operations of facilities including higher temperatures and higher humidity levels.
The looming question moving forward is: How can we accommodate the needs presented by a pandemic while at the same time creating an energy-efficient hospital mechanical system? For years, there has been a goal to design facilities for net-zero operations in 2030, achieved through steps. For hospitals to achieve the goal and assure that the buildings will perform for decades to come, we need to be designing for net-zero operations today.
Chasing 2030
In 2015, the goal at the time was to achieve a 75% reduction from base line. By 2020, the goal was 80%. In Chasing 2030: Mechanical Strategies for Hospitals, our 2015 study evaluated a series of plant and distribution options for a critical access hospital to find a more energy efficient system for heating, cooling, and ventilating hospitals, with the target EUI set at 75 from a baseline of 249 (representing the 75% reduction).
Download the Chasing 2030: Mechanical Strategies Presentation.
Our studies showed that those systems where the ventilation requirements are de-coupled from heating and cooling needs performed the best and achieved the lowest energy use intensity. Chilled beams rose as a plausible solution. The modelling showed that we could reach the reduction target, by using a decoupled system, using active chilled beams in 86% of the hospital, including the patient rooms.
Since the study, conversations with health system facilities personnel revealed that the cleaning requirements for chilled beams are more frequent than anticipated. The manufacturers recommend vacuuming the coils annually, while some facilities are vacuuming the units two or three times a year. Lint and fibers from the linens used in the patient rooms get trapped in the coil system. This has prevented many from using these systems in their facilities.
Efficient Alternatives for Pandemics
What mechanical systems does a hospital require during a pandemic? When looking at isolating patients, as is the case in the current COVID-19 pandemic, patient rooms need to be fully exhausted and maintain a negative pressure during occupancy. To transition into this purge/isolation mode, increased air flows are required and systems that recirculate air by fan or induced flow can’t be used (i.e. active chilled beams or fan coil units). The flexibility required to move into purge mode requires a rethinking of mechanical and planning strategies that will allow for both energy efficiency and isolation.
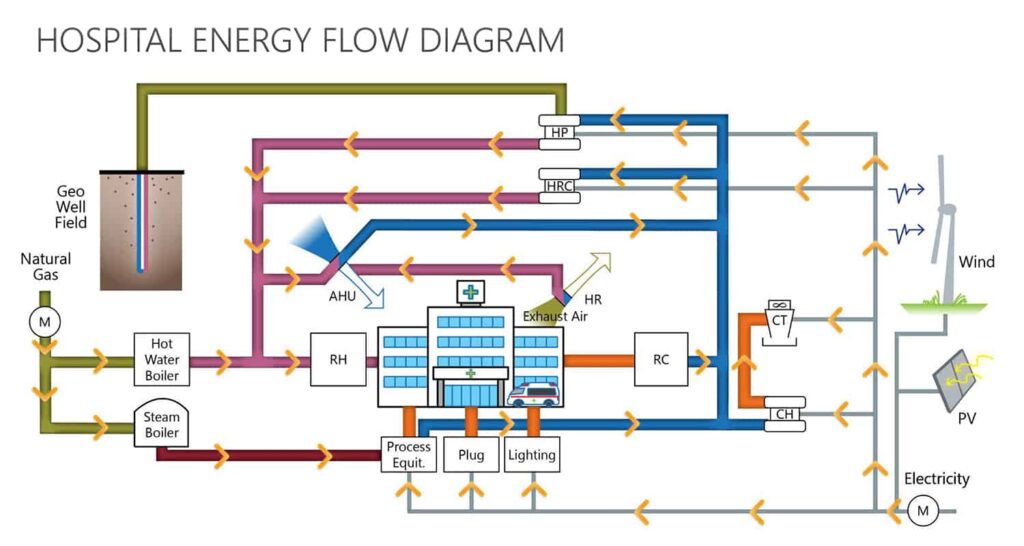
Studies of two alternatives provided data to compare both energy use as well as capital costs for analysis: a DOAS (direct outside air system) unit upstream of a conventional air handling unit (System 1 in this analysis), and a DOAS in parallel with a recirculating air handler (System 2):
- In System 1, dedicated outdoor air and exhaust air fans are used to ensure proper pressurization and flow. Total heat recovery is built into the outside air preconditioning unit.
- In System 2, the DOAS unit includes a total heat recovery system.
Both of these units feed a single terminal box, with 2 dampers and a reheat coil, and for both of these new systems, heat recovery would be suspended during “purge/isolation mode.” Operation during purge/isolation mode matches a typical VAV system to eliminate any possibility for cross contamination between air streams.
In the following energy-use and energy-cost analysis, both System 1 and System 2 are compared to the baseline standard hospital HVAC system consisting of VAV air handling units served by air-cooled chillers and condensing boilers (B1 in the graphics) and system options that were studied in Chasing 2030: Mechanical Strategies for Hospitals: room mounted four pipe fan coils units (B2), displacement four pipe fan coil units (B3), and active chilled beams (B4).
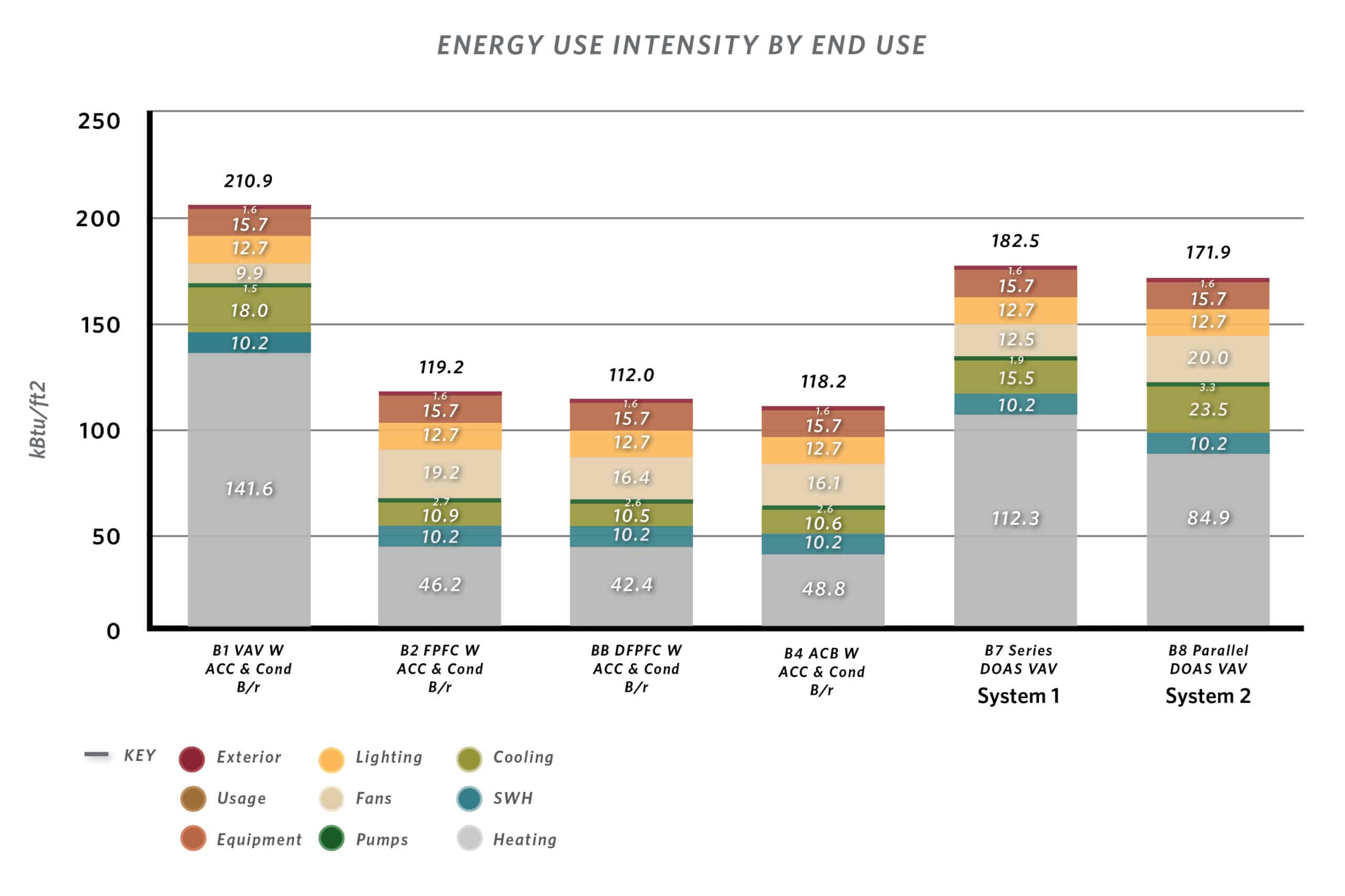
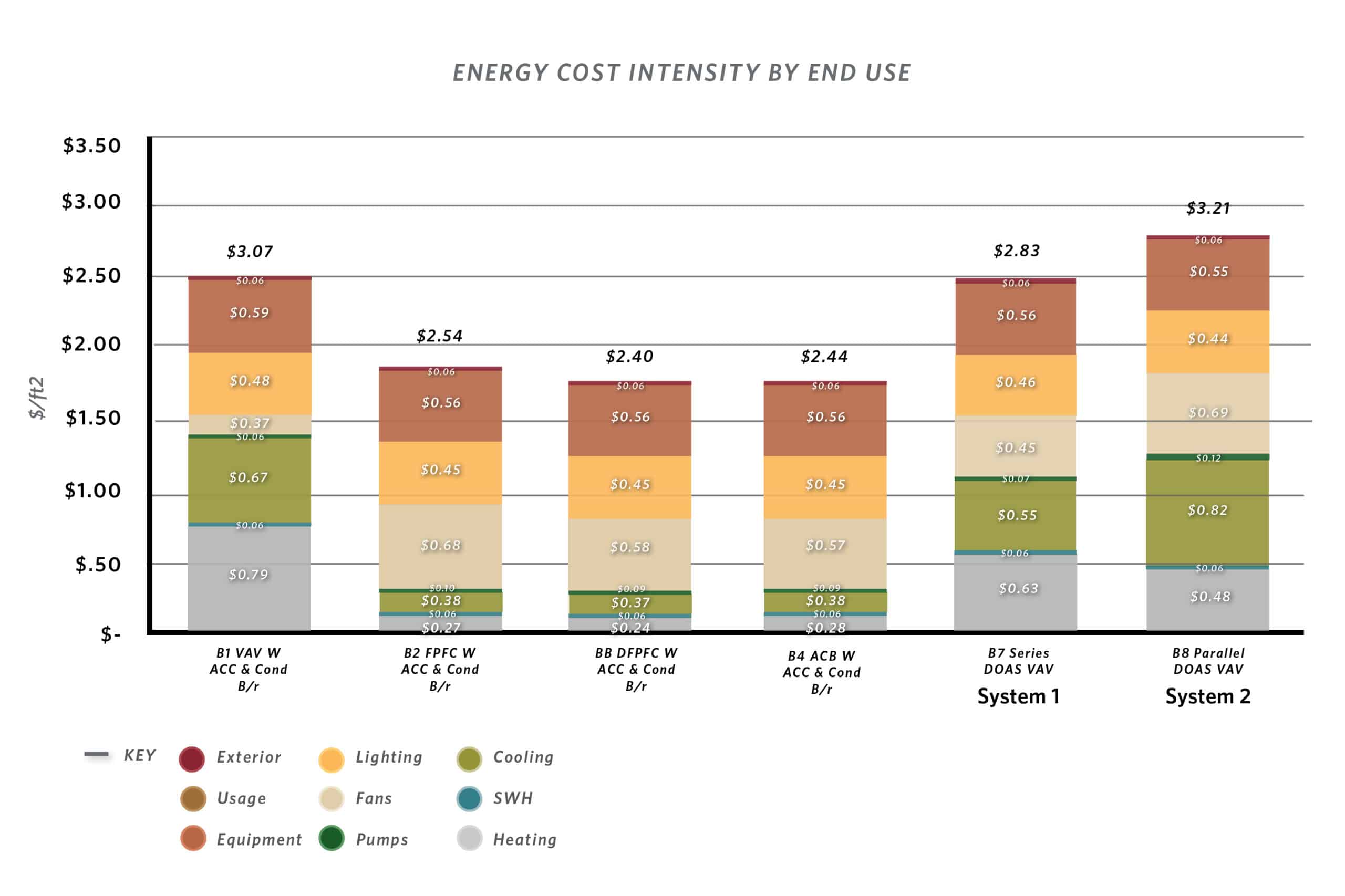
Schematic modelling for System 1 shows a 27% savings over the defined baseline and a 13% savings over the base VAV system. However, due to the added equipment expense and the economy of natural gas over electric power, the system ROI is roughly 30 years.
System 2 shows a 31% savings over the defined baseline and an 18% savings over the base VAV system. However, due to the added equipment expense the economy of natural gas over electric power, the system ROI is never realized.
Treating the Air for Infection
As the analysis indicates, the HVAC system can achieve energy reduction goals, however, it still leaves open the question of how facilities can shift its operations to mitigate infection spread during a pandemic. Solutions to the challenge are both programmatic and mechanical.
On the programming side, identification of space for treatment of infectious patients depends on unique variables according to a facility or system:
- Can a percentage of patient rooms be allocated as “pandemic-capable?” This could be a floor, a wing, or just a few rooms, depending on the size and location of the facility, if not a separate facility specifically identified for treatment of infections patients in a pandemic that allows a health system’s other facilities to remain in normal operations.
- Can a space deploy alternative, decoupled HVAC systems? This could depend on a facility’s size that warrants several air-handling system types, or a scale of a split appropriate for two separate HVAC systems.
- Can a facility accommodate a full exhaust system for pandemic inpatient care areas, and use air treatment systems for outpatient, office, and transient spaces?
- Can areas be zoned for pandemic operations, specifying the air handling systems accordingly?
Many of these questions are easier to answer when designing a new facility versus renovating one. However, for renovations or expansion, there are programming possibilities:
- Converting to or adding pandemic-ready rooms.
- Evaluating what a pandemic-mode operation looks like to understand if the existing infrastructure can support full exhaust systems and whether N+1 heating capacity can address the additional heating loads required.
- Retrofitting the air treatment systems into existing HVAC for outpatient, support, and other transient spaces.
On the mechanical side, tried solutions as well as new applications have opened a world of options for facility managers, all with their relative benefits and costs:
Full Exhaust Systems: Full exhaust systems are best to provide for patients who have tested positive and are contagious. A full exhaust system will prevent spread of the virus through the HVAC system and, by keeping the patient care room in a negative pressure, the virus is prevented from moving with the room pressurization to other locations within the facility. However, the HVAC system will not significantly change the path within the room of the virus particles when aspirated (cough, sneeze) by the patient, so others in the same room are not protected from the contagious patient.
Bipolar Ionization: This is a relatively new application for a technology that has been in the industry for a short time. Bipolar Ionization generates ions at the central air handling system that are discharged throughout the distribution system of the air handling unit. The ions will attack the protein shell of the virus and deactivate them.
As the efficiency of this system in discharging ions into the space and the timing of deactivation in an active space is unknown, the best application for this type of system is in a space where there are no known positive cases but where several people (patient, visitors, and staff) are moving throughout the space that could possibly be aspirating active virus cells into the space. With these ions being distributed by the air handling system they are effectively treating the HVAC air stream and the space where the air is discharged. This technology also is effective on mold, bacteria, and VOCs, contributing to a healthier environment.
Ultra Violet Germicidal Irradiation (UVGI): For UVGI to be effective on the COVID-19 virus and other similar viruses it must be in the form of UVC with wave lengths that are effective at neutralizing the virus cells. Since UVC is harmful to people, it must be applied either in an air handling system or in space that is unoccupied.
To be effective in a healthcare environment (24/7 operation) typically this is applied in the air handling unit; however, the virus must pass through the UV array within the air handling unit and spend a long enough duration within the array to be neutralized. This technology, while effective, must be reviewed for its limitations.
Air Filtration: Minimum air filtration guidelines are presented by ASHRAE 170 for healthcare HVAC systems. The minimum rating of the final filters in an HVAC system is MERV 14. To be effective on COVID-19 the rating should be MERV 17 (HEPA). With the particle size of COVID-19 being between 0.07 to 0.12 micron, a HEPA filter is only approximately 80% effective on this particle size. Air filtration also requires the virus to be airborne from the space through the return air system back to the unit to be captured. Air filtration does not treat virus particles within the occupied space.
Humidity: Relative humidity impacts the distance at which the virus can be transmitted through aspiration. In typical spaces, safe distance has been documented at six feet. With an increase in the relative humidity level to between 40% and 60%, studies show that distance reduces to four feet or less. While this is an improvement, the building envelope could form mold based on typical design practices depending on the outside air temperature that could lead to moisture within the exterior wall.
Multifaceted Solution
When COVID-19 spread, the challenge for healthcare facilities was to implement CDC recommendations to care for the surge of patients with the coronavirus. Actions required a patient room strategy and spaces that mitigated the spread of the virus during patient treatment. Evaluating existing HVAC systems, active chilled beam and fan coil unit patient rooms were incapable of being converted into negative pressure rooms due to the room air being recirculated within the patient room.
While the expected surge has morphed into a state of managed intense operations, the idea that pandemic operations will only ebb and flow as corona and other viruses increase in frequency is redefining normal operations for hospital and health systems. Managing the pandemic is evolving into managing the resiliency of operations to mitigate the impact of a pandemic.
A substantial percentage of the operational budget of the facility is in the utilities to support the HVAC systems, presenting one of the larger opportunities for facilities to manage both its costs as well as its capabilities to continually serve patients no matter the stresses in the community. Reliability and safety have always led the design of the HVAC system. COVID-19 has now made flexibility an equal imperative.
Yet, even as the pandemic has redefined what is consider normal operations, sustainability still must be a focus, both for cost efficiency and the health of the community. While seemingly a pursuit for a unicorn of a solution, the analysis of HVAC systems that can achieve cost savings will also serving various operational needs is more a search for a team of stallions that can work in unison. The HVAC system goes a long way to achieving our energy reduction goals as part of a comprehensive solution, including the building envelope, lighting, plug loads, and on-site renewable energy production.
No one can predict accurately the duration of the pandemic or when the next one will occur and understanding the role the HVAC system will play in the transmission will be ever evolving, especially as each novel virus will present different challenges. What is known is that HVAC systems will predominantly operate in a defined normal mode over the life of the system. Designing the system to help facilities operate at their most optimal efficiency with an eye towards a future of adverse operations will have the biggest benefit ensuring hospitals can navigate a pandemic effectively and resiliently.





